Introduction to
Interventional Pain Management
Oliver Ghalambor, MD, DABA, FIPP, DABIPP, DABPM
Frequency of Pain
- 3 out of 4 people have experienced chronic/ recurring pain or have a family member who has experienced such pain
- Almost 62% of pain sufferers have had their pain for more than a year
- A majority of adults (57%) have experience chronic or recurring pain including 54% of patients between 18-34
Raising Pain Awareness
- 50 million Americans are partially or totally disabled from chronic pain
- 9 out of 10 Americans (18 or older) suffer with pain at least once a month
- 50% of Americans (65 or older) suffer with pain on a daily basis

Back Pain
- Affects 2/3 of adults
- 2nd most common reason for physician visit
- Most common reason for work disability
Why do we have back pain?
One theory as to why humans have so many spine and especially low back problems hypothesizes that vertebrates were never meant to be upright. Humans for the most part are the only vertebrates that constantly load their spinal structures vertically and hence they experience more troubles with their spine than their non-upright vertebrate counterparts. But this is just a theory!
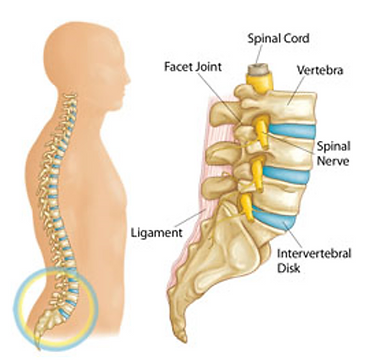
Spine Structures
A quick review of the spinal structures will help one understand what can go wrong with the spine. The discs can get in trouble by the jelly of the disc (nucleus) coming out (herniation) or by the disc simply getting worn out (degeneration). The joints of the spine (facet) joints can also get worn out and get arthritis. The bones (vertebrae) can break, especially if they are fragile (osteoporosis) and finally the surrounding tissues such as muscles, tendons, and ligaments can get damaged (usually short term) which we call sprain/ strain.
Spine Structures
- Disc > Degeneration/ Herniation
- Joints > Arthritis
- Bone > Compression Fracture
- Ligaments and Tendons > Sprain/ Strain
Xray of the Lumbar Spine
Left: Normal Disc Height
Right: Disk Degeneration
Disk Herniation (Different types)
- Disc material (Nucleus Pulposus) is a gelly like substance within the outer lining of the disc (Annulus Fibrosus). Like a Jelly Donut!
- If the Jelly leaks out, it becomes a highly irritant material, setting the area on fire (inflammation).
- When it touches the neighboring nerves, it can irritate and even damage them, causing Sciatica.
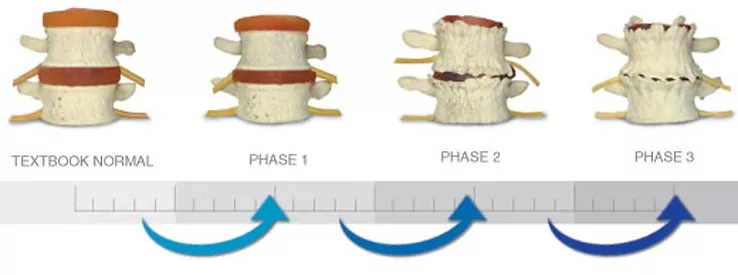
Disk Degeneration (Different Phases)
- When there is less Jelly in the disc, it will dry out and collapse, called disc degeneration.
- On the X ray, it would look like the bones are closer to each other.
Athritis (of the facet joints)
- The joints of the spine are called "Facet" joints.
- Like any other joint in the body, the facet joints can have "wear and tear" called arthritis, and become painful.
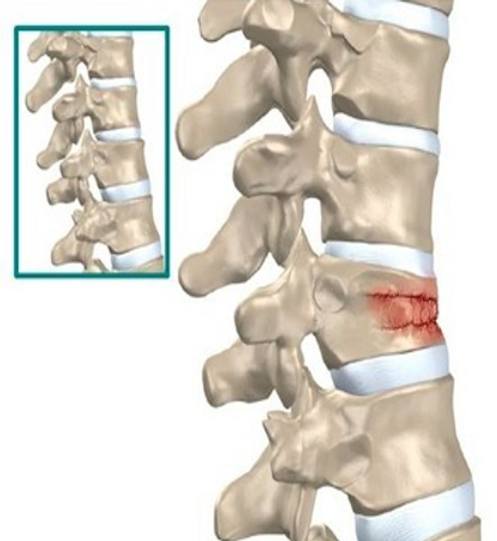
Compression Fracture
- The bones of the spine "Vertebrae" can break.
- This usually happens either when there is a big trauma (Traumatic) like being involved in a Motor Vehicle Accident; or when the bone has become fragile (Osteoporosis).
Risk Factors/ Preventions
- Familial Trends/ Genetics
- Smoking
- Alcohol
- Excess Body Weight
- Repetitive Strain & Vibration
- Pregnancy
- Poor Body Posture
- Not enough Calcium and Vitamin D
The main question here is what can one do to avoid having spine problems. Otherwise said, what are the “risk factors” and how can we avoid getting in trouble with our back or neck.
Based on what research has found, the most frequent reason why one has back or neck problems is determined by their genetic. So watch out if your father and mother have spine related issues. Also, we have found that excessive body weight, smoking, excessive drinking, poor body posture, jobs that are too hard on the body such as Truck driving or Jack Hammer operation call all lead to accelerated wear and tear of the spine.
Prevention therefore, should focus of smoking cessation, being cautious with duties that overload the spine, keep the muscles especially core body muscles in good shape to support the spine while keeping an eye on your calories.
Being conscientious about your posture, especially if you are in front of the computer, or using electronics in your hands with you head bent down “Tech Neck” are good preventative advises.
Lastly, supplementation with Calcium and Vit D. especially in post menopausal periods has been shown to help prevent osteoporosis and therefore compression fractures.
Spine Structures
- Disc > Degeneration/ Herniation
- Joints > Arthritis
- Bone > Compression Fracture
- Ligaments and Tendons > Sprain/ Strain
Since the disc does not have any vascular supply, the anti-inflammatory medications (steroids) need to be delivered close to the area of inflammation which is the epidural space.
Interlaminar Epidural Steroid Injection
The oldest and easiest way to inject steroids in the epidural space is via the interlaminar approach. This could be done without Xray.
However, most of the medication will remain in the posterior epidural space or will travel to the path of least resistance which is the normal side; and therefore can be less efficacious.
Summary of Pain Management Interventions
While the best way to deal with spine and joint related problems is to avoid them (prevention); unfortunately most of the time we see patients after the problem has already started and therefore needs to be treated before we can talk about prevention.
The good news is, over the course of last 20-30 years we have made tremendous amount of improvement for the spine and joint related problems. It is no longer “get it some rest”, “do some physical therapy” and then straight to the surgeon’s office.
At this point in time, the Interventional Pain Management has become a specialty requiring most physician to do a fellowship and get board certification in order to be able to offer most advanced non surgical treatments for back, neck and joint problems.
I have done my best to summarize some of the most frequently offered treatment for each problem we described above. The list is by no means comprehensive. To learn more about some of the available treatments, you can click on the “Treatments” tab of this website.
Transforaminal Epidural Steroid Injection
The injection of steroids in the epidural space via transforminal approach is more precise and results in better delivery of the medication at the site of inflammation. This needs to be done under fluoroscopy and with use of contrast and requires more training and skills.
Disc Herniations Unresponsive to Injections
Not all disc herniations will respond favorably to conservative management including epidural steroid injection.
Old Approach: Big Surgery
The rather old approach to disc herniations that are unresponsive to epidural steroid injections is to remove the disc surgically via an open discectomy. Unfortunately, most of times in order to reach the disc one needs to remove bony structures such as lamina and facet joints resulting in the instability of the spine. And therefore, the structural integrity of the spine would need to be re established using hardware and fusion. The outcomes are often times disappointing.
New Approach
Ultra Mimimally Invasive Endoscopic Discectomy
Thanks to the advances in the medical technology, it is now possible to reach the disc herniation and remove it via the foramen, negating the need for open surgery and removal of the bone. This is called an “Ultra” minimally invasive surgery.
Spine Structures
- Disc > Degeneration/ Herniation
- Joints > Arthritis
- Bone > Compression Fracture
- Ligaments and Tendons > Sprain/ Strain
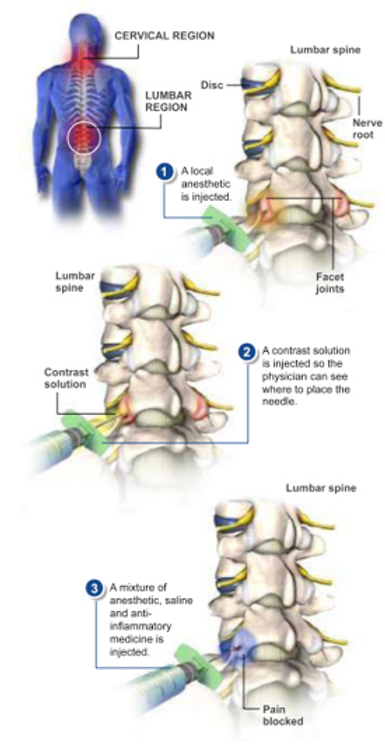
Facet Joint Injection
Facet joint injections are the “arthritis shots” in the neck (cervical spine) or the back (thoracic and lumbar spine).
This is done under fluoroscopy and is done both to help the pain as well as to diagnose/ confirm that the pain is coming from the joints.
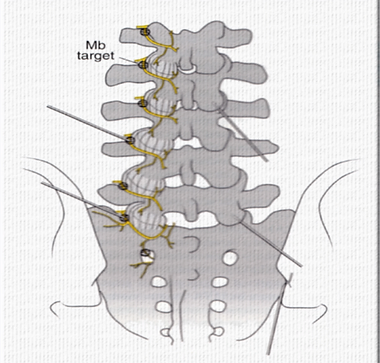
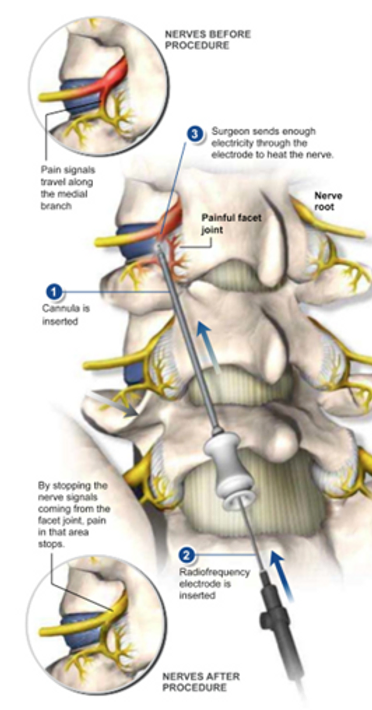
Facet Joint Medial Branches
Anatomical studies have shown that the pain signal from the facet joints travel via small pain “wires” called medial branches. These small nerves have no other function than to bring the pain signals from the joints of the spine.
Lumbar Radiofrequency Neurotomy (Rhizotomy)
If the regular facet injections (spine arthritis shots) fail to provide long term relief, we have the technology to cauterize the medial branches (pain wires) to provide long term relief. This is called radiofrequency neurotomy or rhizotomy.

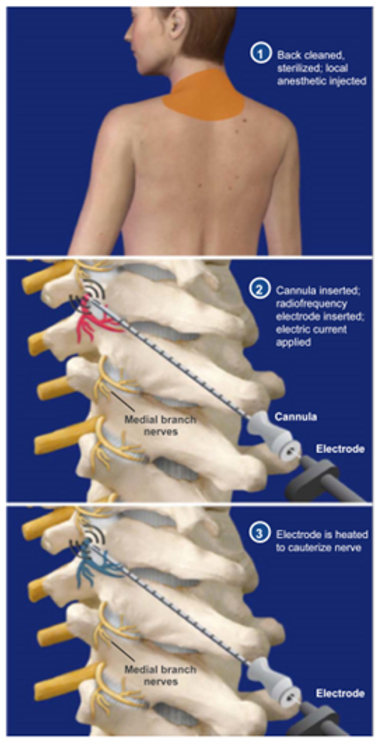
Cervical Epidural Steroid Injection
In a similar manner to the back (lumbar spine) region, disc problems in the neck (cervical spine) region are treated with epidural steroid injections.
Cervical Facet Radiofrequency Neurotomy
In a similar manner to the back (lumbar spine) region, joint problems in the neck (cervical spine) region are treated with facet injections followed by rhizotomy if the joint injections fail to provide long term relief.
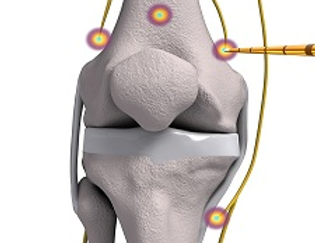
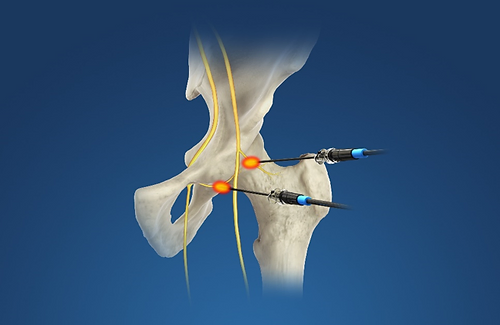
Treatment of ongoing knee pain and hip pain is possible by inactivating pain wires of the knee joint (genicular nerves) as well as the hip joint (femoral and obturator articular branches).
Joint Radiofrequency Neurotomy
Advances in our knowledge about the anatomy of the joints and their pain innervation anatomy as well as medical technological advances have opened the door to treat joint pain for long term.
Spine Structures
- Disc > Degeneration/ Herniation
- Joints > Arthritis
- Bone > Compression Fracture
- Ligaments and Tendons > Sprain/ Strain
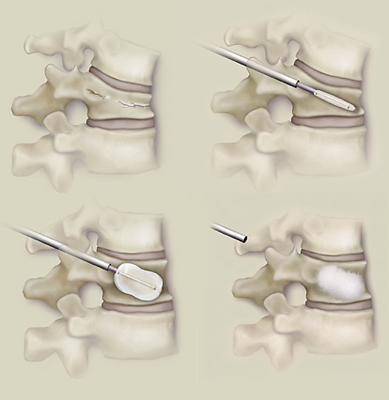
Kyphoplasty Vertebroplasty
Although most painful compression fracture heal on their own, in case of intractable pain, injection of the bone cement in the vertebrae can provide rapid and substantial relief of pain.
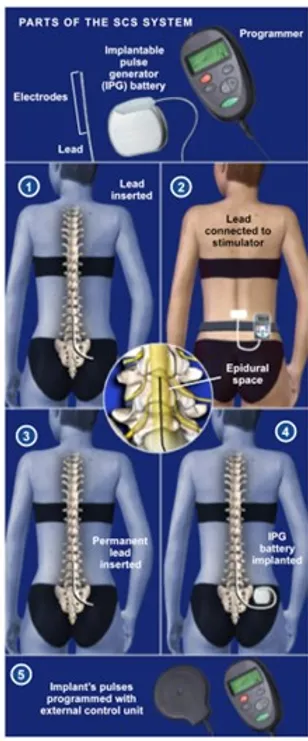
Spinal Cord Stimulation
The idea behind spinal cord stimulation is that if we can no longer treat the painful area; we can modify the signals at the spinal cord level from pain (unpleasant) to massage and tingling (pleasant).
This treatment modality is widely used in cases of failed back surgery syndrome as well as complex regional pain syndrome (RSD).
The advantage of this treatment is that it is first “tested” during trail period by placing the temporary leads via a needle. Only is the trial phase results in significant relief of the symptoms, then the leads and the battery are implanted with a small incision.