Joint degeneration is one of the most common sources of chronic pain in adults, yet it is also one of the most frequently misunderstood conditions seen in clinical practice. Many people assume it is simply an unavoidable consequence of getting older, something to endure rather than address. That assumption leads to delayed care and missed opportunities. Understanding what is joint degeneration at a biological level, recognizing its symptoms early, and knowing which treatments are actually effective can change the course of your condition significantly. This article gives you a clear, clinically grounded explanation of all of it.
Table of Contents
- Key takeaways
- What joint degeneration actually is
- Recognizing the symptoms of joint degeneration
- Causes and risk factors to understand
- How it differs from related conditions
- Joint degeneration treatment options
- My perspective on managing joint degeneration
- Take the next step toward joint relief with Nortexspineandjoint
- FAQ
Key takeaways
| Point | Details |
|---|---|
| More than wear and tear | Joint degeneration involves active biological changes in cartilage, bone, and surrounding tissue. |
| Symptoms vary widely | Stiffness, pain, and reduced range of motion can fluctuate and do not always match imaging findings. |
| Causes are modifiable | Age matters, but weight, movement patterns, and muscle strength also influence disease progression. |
| Not all joint conditions are the same | Degenerative joint disease, degenerative disc disease, and rheumatoid arthritis have distinct mechanisms requiring different treatments. |
| Non-surgical options are effective | Physical therapy, regenerative medicine, and lifestyle changes can meaningfully reduce pain and restore function. |
What joint degeneration actually is
Joint degeneration refers to the gradual structural breakdown of the tissues that make a joint function smoothly. The process centers on cartilage, the firm, rubbery tissue that covers the ends of bones inside a joint. Healthy cartilage acts as a shock absorber and creates a low-friction surface that allows bones to glide past each other. When degeneration begins, cartilage softens and cracks, losing both its thickness and its ability to distribute load evenly.
The body attempts to repair this damage, but those repair processes are imperfect. Bone beneath the thinning cartilage becomes denser and harder, and bony outgrowths called osteophytes, more commonly known as bone spurs, begin to form along joint margins. These spurs can press on nearby nerves or restrict movement. The joint capsule and synovium, the tissue that lines the joint and produces lubricating fluid, also become involved. Inflammation intermittently flares during the body’s repeated cycles of attempting to repair damaged tissue, contributing to pain and swelling.
The distinction between degeneration and purely inflammatory joint disease is clinically meaningful. Degenerative joint disease is a mechanical process at its core, driven by structural failure rather than an immune system attack on joint tissue. That distinction shapes every treatment decision.
Key structures affected during joint degeneration include:
- Articular cartilage: Loses thickness, elasticity, and surface integrity over time
- Subchondral bone: Thickens and may develop cysts or spurs beneath the cartilage surface
- Synovial membrane: Can become mildly inflamed, producing excess fluid and joint swelling
- Ligaments and tendons: Gradually lose their mechanical support capacity around a degenerating joint
Pro Tip: If your physician shows you an X-ray with “joint space narrowing,” they are visualizing cartilage loss indirectly. Cartilage does not appear on standard X-rays; what you are seeing is the reduced space between two bones where cartilage used to provide cushion.
Recognizing the symptoms of joint degeneration
The symptoms of joint degeneration tend to develop slowly and often go unnoticed until they are significant enough to interfere with daily activity. Morning stiffness, joint tenderness, and reduced flexibility are hallmark presentations. That stiffness typically lasts less than 30 minutes after waking, which is one clinical feature that separates degenerative disease from inflammatory arthritis, where morning stiffness often persists much longer.
Pain in degenerative joint conditions generally worsens with activity and improves with rest, at least in earlier stages. Over time, discomfort may persist even at rest. Many patients describe a deep, aching quality rather than sharp pain, and they often notice a grating or clicking sensation in the joint, known as crepitus, when moving.

One detail that surprises many patients: imaging findings do not reliably predict how much pain you experience. Nearly all individuals by age 80 show radiographic evidence of joint degeneration, but only about half report meaningful symptoms. This means two people with identical X-rays can have vastly different pain levels. Your symptoms, not your scan, are the primary guide to treatment decisions.
Common symptom patterns seen clinically include:
- Deep aching pain in one or a few joints, most often the knees, hips, hands, or spine
- Stiffness after periods of inactivity that loosens with gentle movement
- A reduced range of motion that makes tasks like squatting, reaching, or gripping harder
- Occasional swelling around the affected joint, particularly after physical exertion
Pro Tip: If your joint stiffness lasts more than 45 minutes in the morning, or if you notice swelling in multiple joints simultaneously, those patterns warrant a clinical evaluation. They may indicate an inflammatory condition rather than purely degenerative disease, and the treatment pathways are meaningfully different.
Causes and risk factors to understand
Understanding what drives joint degeneration matters because several of the most significant risk factors are ones you can influence. Age is the dominant factor. Nearly 25% of adults over 40 live with symptomatic osteoarthritis, the most common form of degenerative joint disease. The biological explanation is straightforward: cartilage repair capacity declines with age, while cumulative mechanical stress on joints increases over decades.
The key causes and modifiable risk factors, in order of clinical significance, are:
- Age and reduced cartilage repair capacity: Chondrocytes, the cells responsible for maintaining cartilage, become less efficient with age, making tissue regeneration slower and less complete.
- Prior joint injury: A ligament tear, fracture, or significant sprain alters joint mechanics, placing abnormal stress on cartilage surfaces and accelerating breakdown. Post-traumatic arthritis is a well-documented consequence of earlier injury.
- Excess body weight: Every additional pound of body weight places roughly four pounds of force on the knee joint during walking. Weight reduction is one of the few interventions with clear evidence for slowing progression.
- Repetitive mechanical stress: Occupations or sports requiring repeated high-impact movement or sustained joint loading increase cumulative wear on cartilage over time.
- Genetic predisposition: Family history contributes meaningfully to who develops significant degeneration and at what age, though genetic risk is not destiny.
Lifestyle factors like weight management and muscle strengthening can alter the course of the disease even after a diagnosis is made. This is not a hopeful exaggeration. It reflects what clinical evidence and patient outcomes consistently show. Joint degeneration is not simply inevitable or fixed at the moment you receive a diagnosis.
How it differs from related conditions
One of the most common sources of confusion is the overlap in terminology between related joint and spine conditions. Understanding the distinctions prevents mismanagement and helps you ask better questions of your care team.
Degenerative joint disease describes a group of conditions affecting joints rather than a single disease entity. Osteoarthritis is the most prevalent form, characterized by localized cartilage breakdown in one or several joints. It is a mechanical process, not an immune-mediated one.
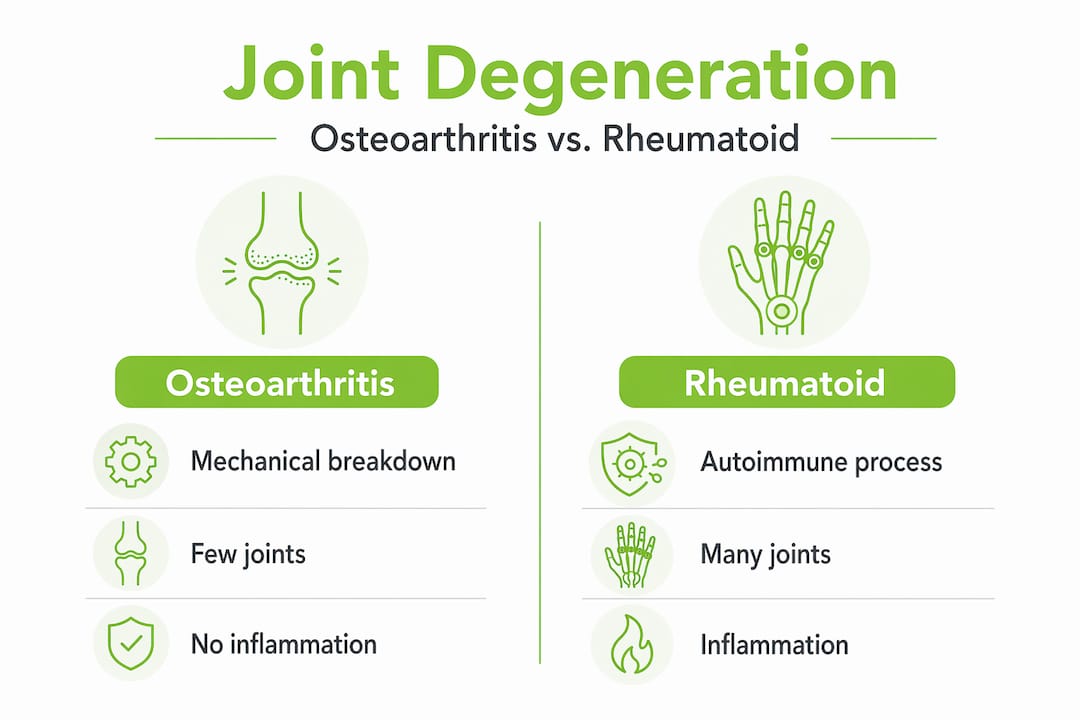
Rheumatoid arthritis (RA) is categorically different. RA is an autoimmune systemic disease in which the immune system attacks the synovial lining of joints throughout the body. It is symmetric, systemic, and driven by immune dysfunction rather than mechanical wear. The treatment protocols are entirely distinct, relying on disease-modifying drugs rather than the biomechanical or regenerative approaches used for osteoarthritis.
Degenerative disc disease is a related but separate process affecting the intervertebral discs of the spine. Discs lose hydration, height, and structural integrity with age, leading to back or neck pain. It frequently coexists with facet joint degeneration in the spine, but it involves disc tissue rather than the hyaline cartilage of peripheral joints like the knee or hip.
| Condition | Mechanism | Joint involvement | Key features |
|---|---|---|---|
| Osteoarthritis | Mechanical cartilage breakdown | Localized, asymmetric | Pain worsens with activity, bone spurs |
| Rheumatoid arthritis | Autoimmune synovial attack | Symmetric, systemic | Prolonged morning stiffness, systemic symptoms |
| Degenerative disc disease | Disc dehydration and height loss | Spinal segments | Back or neck pain, radiculopathy possible |
Radiographic findings alone do not predict symptom severity in any of these conditions. Professional clinical diagnosis, informed by history, physical examination, and imaging together, is what guides appropriate care.
Joint degeneration treatment options
Treatment for joint degeneration works best when it targets the specific mechanisms driving your symptoms rather than applying a generic protocol. Many patients arrive after trying multiple approaches that provided only partial or temporary relief, which is often a sign that the root cause, whether biomechanical, inflammatory, or structural, has not yet been fully addressed.
Effective options by category:
- Physical therapy and gait modification: Personalized biomechanical interventions, including specific gait retraining, can reduce joint loading and relieve pain comparably to medication in some patients. Targeted exercise preserves muscle support around the joint, which is the most durable form of mechanical protection cartilage can receive. For more on this, see how physical therapy for arthritis can specifically help.
- Weight management: Even modest reductions in body weight produce disproportionate reductions in joint loading forces, particularly at the knee and hip.
- Medications: Nonsteroidal anti-inflammatory drugs (NSAIDs) and topical analgesics address pain and acute flares but do not alter disease progression. Corticosteroid injections offer temporary relief and are best reserved for acute exacerbations rather than long-term management.
- Regenerative medicine: PRP (platelet-rich plasma) therapy and stem cell treatments target the biological environment of the joint, supporting tissue repair and reducing inflammation at the source. These are particularly relevant for patients who have not responded adequately to conservative measures but wish to avoid surgery.
- Surgical intervention: Joint replacement or debridement may become appropriate when degeneration is severe and function is substantially compromised. Surgery is most effective when conservative and regenerative options have been explored first.
You can read more about non-surgical joint health strategies to understand how these approaches fit together into a cohesive plan.
Pro Tip: Starting physical therapy before your joint pain becomes severe is significantly more effective than beginning it after significant muscle atrophy and compensatory movement patterns have developed. Earlier is better, consistently.
My perspective on managing joint degeneration
I’ve seen the “wear and tear” label do real harm to patients. It implies passivity, as though the body is simply breaking down and there is little to be done. In my clinical experience, this framing discourages patients from pursuing interventions that could genuinely change their trajectory.
What I’ve found is that joint degeneration is far more responsive to targeted intervention than most patients expect. The patients who do best are those who understand their specific biomechanical deficits, address them with focused physical therapy, and pursue regenerative options early rather than waiting until surgery feels unavoidable. I’ve watched people regain mobility they assumed was permanently lost, not through dramatic procedures, but through precise, consistent, individualized care.
The most important thing I would want you to take away is this: your imaging results are not your destiny. They are one data point. What matters more is how your joint functions, how your muscles support it, and what biological environment surrounds it. Those are all things we can work with. Realistic expectations are important, and meaningful improvement is possible for most people who engage proactively.
— Felix
Take the next step toward joint relief with Nortexspineandjoint
At Nortexspineandjoint, we specialize in non-surgical solutions for chronic joint pain rooted in evidence-based regenerative medicine. If you are living with the symptoms described in this article, you do not have to simply manage them with medication alone. Our PRP therapy for joint pain uses your body’s own growth factors to reduce inflammation and support tissue repair at the cellular level. For more advanced cases, we also offer stem cell therapy as part of a personalized treatment plan. Every patient at our North Dallas clinic receives a thorough evaluation to identify the actual drivers of their pain, not just a standard protocol. Contact us to schedule a consultation and explore what targeted, individualized care can do for your joints.
FAQ
What is joint degeneration in simple terms?
Joint degeneration is the gradual breakdown of cartilage and surrounding joint structures, leading to pain, stiffness, and reduced mobility. It is most commonly associated with osteoarthritis and progresses over time as the body’s repair capacity declines.
What are the earliest symptoms of joint degeneration?
Morning stiffness lasting less than 30 minutes, a deep aching pain that worsens with activity, and a grating sensation in the joint are typically the earliest signs. Many people also notice a gradual reduction in their range of motion before significant pain develops.
How is degenerative joint disease different from rheumatoid arthritis?
Degenerative joint disease is a localized mechanical process involving cartilage breakdown, while rheumatoid arthritis is a systemic autoimmune condition that attacks the joint lining throughout the body. The distinction is critical because each condition requires a different treatment approach.
Can joint degeneration be stopped or reversed?
Degeneration cannot be fully reversed, but its progression can be meaningfully slowed through weight management, targeted exercise, and regenerative treatments. Many patients experience significant pain reduction and functional improvement with the right combination of interventions.
What is degenerative disc disease and how does it relate to joint degeneration?
Degenerative disc disease involves age-related changes to the spinal discs, including dehydration and height loss, rather than breakdown of hyaline cartilage in peripheral joints. The two conditions often coexist in the spine but represent distinct tissue changes requiring individually tailored treatment plans.






{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}